While early symptoms of rheumatoid arthritis can actually be mimicked by other diseases, the symptoms are very characteristic of rheumatoid disease. Rheumatoid arthritis symptoms and signs include the following:
Fatigue
Fatigue is a very common symptom in all stages of rheumatoid arthritis, particularly when the joint inflammation is active. Fatigue in rheumatoid arthritis can be caused by the body’s reaction to inflammation, poor sleep, anemia, and medications.
The fatigue of rheumatoid arthritis that results in lack of energy can adversely affect emotions and mood, occupation, relationships with people, sex drive, productivity, attentiveness, creativity, and happiness. Fatigue from rheumatoid arthritis can also be associated with poor appetite and weight loss.
Joint pain
Joint pain from rheumatoid arthritis is caused by the inflammation present in a joint when the disease is active. Joint pain can also occur when the disease is inactive or controlled if the joint has been damaged by rheumatoid arthritis in the past.
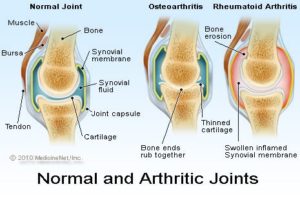
Active rheumatoid arthritis causes the joint to swell because of both thickening of the joint lining tissue (synovium) and because of excess joint fluid. The swollen, inflamed joint stretches and irritates the capsule that surrounds the joint. The joint capsule has nerves endings within it that immediately send pain signals to the brain.
Past rheumatoid arthritis can lead to permanent joint destruction with damaged cartilage, bone, and ligaments. When the damaged joint is used, it can cause intense pain.
Joint tenderness
Rheumatoid arthritis characteristically leads to tenderness of involved joints. This is because the inflamed joint lining tissue has irritated the nerves in the joint capsule. When the irritated joint capsule is compressed by external pressure, such as from touching the joint, it is frequently tender. The pain elicited from compression is immediate. This is one of the reasons that rheumatoid arthritis can lead to difficulty sleeping and insomnia.
Joint swelling
Swollen joints are very common in rheumatoid arthritis. Sometimes the joint swelling is minimal and can be difficult to appreciate. Other times the joint swelling is very apparent. Generally, people who are affected by rheumatoid arthritis can easily tell when their joints are swollen. The joint swelling can lead to loss of range of motion of the joint. Joint swelling in the fingers can make it hard to get rings off and on easily.
Joint redness
Redness occurs over joints when they are inflamed. The redness in the skin over an inflamed joint from rheumatoid arthritis occurs because the capillaries of that skin are widened by the adjacent inflammation. These widened capillaries are referred to as dilated capillaries.Joint redness does not occur in all inflamed joints from rheumatoid arthritis. Sometimes the inflammation in the joint is inadequate to cause the capillaries in the skin to dilate.
Joint warmth
Warmth of the joints affected by rheumatoid arthritis is a sign of active inflammation. Doctors look for joint warmth as they monitor the activity of the disease. As rheumatoid arthritis responds to treatment, joint warmth resolves. Sometimes joint warmth is present without visible joint swelling or redness.
Joint stiffness
Stiffness is a typical rheumatoid arthritis symptom. Joints that are affected by active rheumatoid arthritis are inflamed and characteristically stiffer in the morning than later in the day. Doctors use the duration of the morning stiffness as a measure of the severity of the active joint inflammation. As rheumatoid arthritis responds to treatment, the duration of the morning joint stiffness diminishes.
Loss of joint range of motion
As the joints of rheumatoid arthritis become more inflamed with active disease, they tend to have incomplete range of motion. The range of motion is limited by the swelling within the joint. This is typically associated with weakness in the involved areas.
Joints affected by longstanding rheumatoid arthritis commonly lose range of motion permanently.
Limping
Limping from poor lower extremity function can be caused by many diseases of the nerves, muscles, and bones of the lower extremities. Limping frequently occurs when rheumatoid arthritis affects the hips, knees, ankles, or feet. Pain, loss of range of motion, and joint swelling all can cause a person with rheumatoid arthritis to have a noticeable limp. It is not unusual for a young child with rheumatoid arthritis to have a painless limp as the first sign of the rheumatoid disease.
Joint deformity
Joint deformity can occur from chronic rheumatoid arthritis. Deformity in rheumatoid arthritis occurs because the unchecked inflammation leads to both erosion of cartilage and bone as well as ligament loosening (laxity). Early detection and treatment of rheumatoid arthritis is critical to prevent permanent joint destruction and joint deformity.
Many joints affected (polyarthritis)
Usually, but not always, rheumatoid arthritis affects many joints. Classically, RA affects the small joints of the hands and wrists and balls of the feet. Also, not uncommonly, knees, elbows, hips, ankles, and shoulders can be inflamed.
Sometimes, only a few joints are involved. Less frequently, a singular joint is involved. Both of these scenarios are more common in childhood inflammatory arthritis (juvenile rheumatoid arthritis).
When four or more joints are inflamed, the condition is referred to as polyarthritis. When only a few joints are inflamed, it is referred to as oligoarthritis. When a single joint is inflamed, it is referred to as monoarthritis.
Both sides of the body affected (symmetric)
Typically, the distribution of the joints involved in a person with rheumatoid arthritis is similar on both sides of the body. This symmetric joint involvement is a feature of classic rheumatoid arthritis. This does not mean that joint involvement is always symmetric, but it is common.
Rheumatoid arthritis usually (not always) involves many joints on both sides of the body. It is, therefore, sometimes referred to as a symmetric polyarticular form of arthritis. Accordingly, the small joints of the hands, wrists, and feet are commonly affected. The knees, ankles, shoulders, hips, and elbows can also be involved in early disease. Rheumatoid arthritis is characterized by inflammation in these joints. Early manifestations of this inflammation can be gradual or rapidly intense. The joint inflammation causes stiffness, usually worse in the morning or after being sedentary. It also causes warmth, swelling, redness, and pain in varying degrees. The joint can be very subtly affected with slight swelling or markedly affected with substantial loss of range of motion. The pain level can be completely disabling and does not always correlate with the degree of apparent inflammation.
As described above, the manner that each of the symptoms affects an individual can be very different from individual to individual and can vary during the day. The intensity and effect of each of the symptoms is dependent upon the patient’s age, activity, the medications he or she takes, as well as any additional medical conditions that are present.
Loss of joint function
Because rheumatoid arthritis leads to pain, swelling, and tenderness of the involved joints, there is loss of joint function. The swelling and sensitivity impedes the full motion and stability of the joint and it becomes incapable of carrying the movement with confidence, balance, and completeness. This loss of joint function leads to limping, lack of coordination, loss of grip and dexterity, and disability.
Anemia
The chronic inflammation of rheumatoid arthritis commonly causes the bone marrow to decrease the release of red blood cells into the circulation. This lowers the red blood count to cause anemia when rheumatoid arthritis is active. It is not unusual for the anemia of rheumatoid arthritis to spontaneously correct as the inflammation of the disease is quieted by treatment.
Fever
Fever, while not common in rheumatoid arthritis, does occur in some patients when the disease is actively causing inflammation. Typically, there is only mild low-grade temperature elevation and this corrects rapidly as the inflammation of rheumatoid arthritis is treated. Because patients with rheumatoid arthritis frequently require medications that can decrease the normal immune response, it is important that when they develop fever, infection is considered as a possible cause. Infections can require aggressive treatment and interruption of some underlying rheumatoid treatments.

 Chinese Herbal Medicine includes: medicine, relieving drugs, Qingre drugs, temperature in medicine, Qi drugs, drug Xiaoshi close, Shibuya medicine, medicine Huashi aromatic medicine, medicine diuresis, Ping asthma drugs, sedative drugs, medicines wind Pinggan intake, remove silt Huoxue drugs, hemostatic, diarrhea medicine, de-worming medicine and aromatic Kaiqiao medicine.
Chinese Herbal Medicine includes: medicine, relieving drugs, Qingre drugs, temperature in medicine, Qi drugs, drug Xiaoshi close, Shibuya medicine, medicine Huashi aromatic medicine, medicine diuresis, Ping asthma drugs, sedative drugs, medicines wind Pinggan intake, remove silt Huoxue drugs, hemostatic, diarrhea medicine, de-worming medicine and aromatic Kaiqiao medicine. Cupping Therapy is a cup-like device using heat as a means of absorbing negative pressure in the adsorption of the acupuncture points on the skin, causing local congestion, congestion as a method of treating disease.
Cupping Therapy is a cup-like device using heat as a means of absorbing negative pressure in the adsorption of the acupuncture points on the skin, causing local congestion, congestion as a method of treating disease.